What Is a Fertility Workup and Why It Matters
- Feb 22
- 12 min read
Updated: Mar 18

Facing fertility challenges after 35 often sparks more questions than answers, especially when every month brings new hopes and disappointments. Knowing that fertility problems affect about 1 in 6 couples worldwide makes it clear you are not alone, and the path forward starts with understanding, not assumptions. This guide breaks down what a comprehensive fertility workup really involves, uncovers common myths, and empowers you to partner with your specialist for a plan tailored to your needs.
Table of Contents
Key Takeaways
Point | Details |
Comprehensive Evaluation | A fertility workup includes reviewing medical history, physical exams, hormone testing, and family history to identify causes of infertility. |
Timing is Critical | Begin the fertility workup after 12 months of trying (or 6 months if over 35) to ensure timely diagnosis and treatment. |
Dispelling Myths | Common misconceptions about infertility can delay effective treatments; understanding the realities can save time and resources. |
Personalized Treatment Plans | Results from the workup inform tailored fertility strategies, enhancing the chances of successful conception. |
Fertility Workup Basics and Common Myths
A fertility workup isn’t just a single test. It’s a comprehensive evaluation to identify why you’re struggling to conceive. Think of it as detective work—your healthcare provider gathers clues from your history, physical findings, and test results.
If you’ve been trying to conceive for 12 months without success (or 6 months if you’re over 35), a workup becomes valuable. This timeline matters because age affects egg quality and quantity, particularly for women past 35.
What a Fertility Workup Actually Includes
Your workup typically involves:
Medical and reproductive history review—everything from past surgeries to menstrual patterns
Physical examination—assessing reproductive anatomy and overall health
Fertility testing—hormone levels, ovulation checks, imaging, or semen analysis
Family history evaluation—identifying genetic or reproductive patterns
These components work together to reveal the root cause, whether it’s ovulatory disorders, tubal blockages, male factor issues, endometriosis, or unexplained infertility.
Debunking Fertility Myths That Delay Treatment
Misunderstandings about infertility often delay diagnosis. Here are the biggest myths worth addressing:
Myth 1: Infertility is only a woman’s problem. Reality: Fertility problems affect about 1 in 6 couples, often involving both partners. Male factor issues account for roughly 40% of cases.
Myth 2: Age is the only cause of infertility. Many factors matter—PCOS, tubal damage, uterine abnormalities, sperm issues, and more. Age accelerates decline but isn’t the sole factor.
Myth 3: IVF is always the answer. Not true. Depending on your diagnosis, simpler treatments like medication or intrauterine insemination may work.
Myth 4: Weight doesn’t affect fertility. Your weight influences hormone balance and ovulation. Extremes (too high or too low) can impact reproductive function.
Dispelling these myths leads to earlier diagnosis and better treatment outcomes. You may need fewer interventions than expected once you know your actual diagnosis.
Knowing the truth about fertility saves time, money, and emotional energy—all resources you need for your journey.
Why Timing Matters for Your Workup
Starting a workup at the right time increases your chances of success. For women over 35, the 6-month threshold reflects the biological reality: time matters more when diminished ovarian reserve or age-related egg quality becomes relevant. Waiting 12 months could mean missing a critical window.
A thorough workup also prevents unnecessary treatment. When you understand your specific diagnosis—rather than guessing—your fertility specialist can recommend targeted solutions rather than a one-size-fits-all approach.
Pro tip: Bring documentation of any previous reproductive procedures, hormone levels, or ultrasounds to your initial workup appointment—this historical data accelerates diagnosis and prevents redundant testing.
Key Tests Included in a Fertility Workup
A fertility workup relies on specific, targeted tests rather than guesswork. Each test serves a purpose—identifying whether the issue stems from hormone imbalances, egg quality, ovulation problems, sperm quality, or structural issues. The approach follows a logical progression, starting with the least invasive methods.
Hormone Testing: Reading Your Reproductive Signals
Hormone levels reveal how your reproductive system functions. Blood tests measure key hormones at specific times in your cycle.
Critical hormones include:
FSH (follicle-stimulating hormone)—stimulates egg development; high levels may indicate diminished ovarian reserve
LH (luteinizing hormone)—triggers ovulation; imbalances can affect fertility
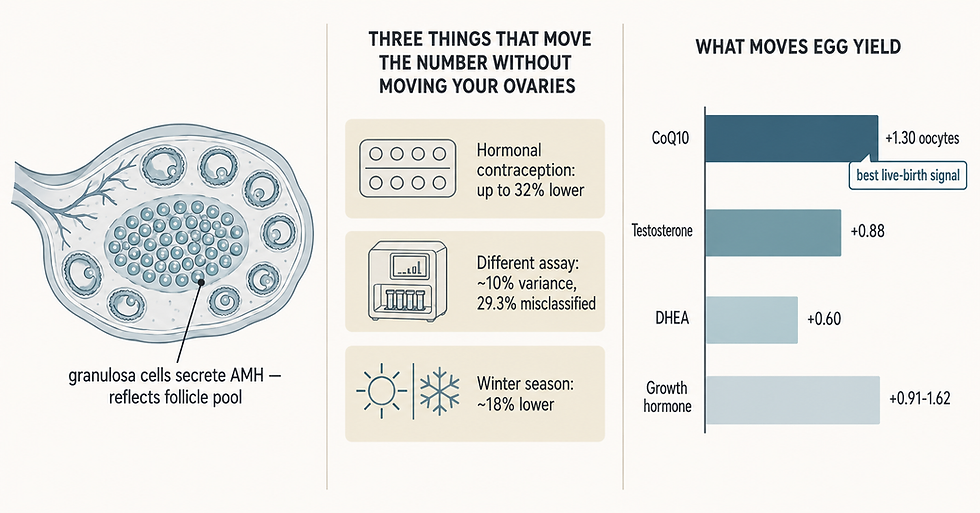
AMH (anti-müllerian hormone)—reflects remaining egg supply; crucial for women over 35
Prolactin—elevated levels can block ovulation
Thyroid hormones—thyroid dysfunction disrupts menstrual cycles and fertility
Estradiol—indicates egg development quality
These tests typically occur on specific days of your cycle for accuracy. Your specialist knows which day to test based on your cycle length.
Ovarian Reserve Assessment: Understanding Your Egg Supply
Ovarian reserve tests answer a critical question: how many viable eggs do you have? This matters enormously for women over 35.
Two main approaches exist:
AMH blood test—measures a hormone produced by developing eggs; lower levels suggest diminished reserve
Antral follicle count (AFC)—ultrasound counts visible follicles in both ovaries; reflects egg supply
Both tests work together. AMH provides a snapshot of hormone levels; AFC shows actual follicles. Neither is perfect alone, but combined they paint an accurate picture of your reproductive capacity.
Semen Analysis: Assessing Male Factor
Semen analysis evaluates sperm quantity, motility (movement), and morphology (shape). Poor sperm health affects roughly 40% of couples dealing with infertility. Sperm evaluation examines count, concentration, and progressive movement—factors that directly impact fertilization chances.

If results show issues, repeat testing often occurs because sperm parameters fluctuate based on lifestyle, stress, and health factors.
Imaging Tests: Visualizing Your Reproductive Organs
Imaging reveals structural problems that blood tests cannot detect.
Transvaginal ultrasound—checks uterine shape, endometrial thickness, and ovarian appearance; non-invasive and quick
Hysterosalpingogram (HSG)—X-ray with dye to visualize fallopian tubes and uterine cavity; detects blockages or abnormalities
Hysteroscopy—surgical camera inside the uterus; used if HSG shows abnormalities or unexplained infertility persists
These tests identify fibroids, polyps, septums, scarring, or blocked tubes—conditions requiring specific interventions.
Here’s a quick comparison of common fertility workup tests and what each reveals:
Test Type | What It Assesses | Why It Matters |
Hormone Bloodwork | Egg supply and ovulation status | Identifies hormonal imbalances |
Ultrasound (AFC) | Number of ovarian follicles | Reflects current egg reserve |
Semen Analysis | Sperm count and quality | Detects male infertility |
HSG Imaging | Fallopian tube openness | Finds blockages or scarring |
Hysteroscopy | Uterine cavity structure | Detects polyps, fibroids |
The most comprehensive fertility evaluation combines multiple diagnostic approaches rather than relying on single tests, ensuring nothing gets missed.
Why This Sequence Matters
Your specialist starts with blood work and ultrasound—affordable, fast, non-invasive. Only if results warrant it do you progress to HSG or other imaging. This cost-effective approach prevents unnecessary procedures while capturing essential information.
Pro tip: Schedule your initial bloodwork between days 2-4 of your cycle for the most accurate FSH and AMH readings—timing affects results significantly.
Assessing Ovarian Reserve and Uterine Health
Two critical components of your fertility workup focus on what you have (eggs) and where they’ll grow (uterus). Both directly impact your chances of conception and successful pregnancy. Understanding these assessments helps you grasp your fertility picture.
Understanding Ovarian Reserve
Ovarian reserve measures your remaining egg quantity and quality. This matters tremendously for women over 35, where egg numbers decline significantly each year.
Two main tests assess this:
AMH (anti-müllerian hormone) blood test—measures a hormone produced by developing eggs; reflects your egg count
Antral follicle count (AFC) via ultrasound—counts visible follicles in both ovaries; directly shows available eggs
AMH testing and follicle counts work together. AMH gives a numerical marker; AFC provides visual confirmation. Neither alone tells the whole story, but combined they predict how many eggs you might retrieve if pursuing fertility treatment.
Lower AMH doesn’t mean pregnancy is impossible—it means timing and treatment strategy become more important. Many women over 35 with diminished ovarian reserve achieve pregnancy with personalized approaches.
What Your AMH Number Means
AMH levels vary, but general ranges include:
Above 1.0 ng/mL—normal reserve for your age
0.5 to 1.0 ng/mL—moderate decline; still viable eggs present
Below 0.5 ng/mL—significantly diminished; fewer eggs available
These numbers guide treatment decisions. Higher AMH suggests conventional IVF may yield more eggs; lower AMH might indicate need for specialized protocols or alternative approaches like ovarian rejuvenation strategies.
Evaluating Uterine Health
Your uterus must be structurally sound for embryo implantation and pregnancy. Several conditions can affect this.
Common issues detected include:
Fibroids—benign muscle tumors that distort the cavity
Polyps—tissue growths that interfere with implantation
Septums—congenital walls dividing the uterus
Scarring (adhesions)—from prior surgery or infection
Uterine shape abnormalities—affecting pregnancy success
Imaging Tests for Uterine Assessment
Uterine abnormalities require specific imaging:
Transvaginal ultrasound—initial screening; non-invasive and quick
Saline infusion sonography (SIS)—ultrasound with saline injected into uterus; shows cavity shape clearly
Hysterosalpingography (HSG)—X-ray with dye; visualizes tubes and cavity
Hysteroscopy—surgical camera inside uterus; allows direct visualization and treatment of problems
Each test serves a purpose. Your specialist decides the sequence based on initial findings. Many issues can be corrected surgically before pursuing fertility treatment.
Addressing uterine abnormalities before treatment significantly improves implantation rates and pregnancy success.
Why Both Assessments Matter Together
You could have excellent ovarian reserve but poor uterine environment—or vice versa. A complete picture requires evaluating both. This comprehensive approach prevents wasted cycles on uterine problems that could be fixed, or pursuing treatment when egg supply isn’t viable.
Pro tip: Request copies of your AMH results and ultrasound images; tracking these over time shows trends and helps guide long-term fertility strategy.
How Results Shape Personalized Fertility Plans
Your workup results aren’t just numbers on a report—they’re the foundation for your personalized treatment strategy. No two fertility journeys look identical, and your plan shouldn’t either. Understanding how clinicians use your specific results empowers you to make informed decisions.
From Diagnosis to Action
Each workup finding points toward targeted solutions. Fertility workup results enable treatment tailoring based on identified causes. Your specialist doesn’t recommend the same treatment for everyone—they match interventions to your diagnosis.
For example, if testing shows ovulation problems, medication to trigger ovulation may suffice. If tubes are blocked, surgery or IVF becomes necessary. Male factor issues require different approaches entirely. This targeted approach saves time and resources.
Common Diagnoses and Their Solutions
Here’s how specific findings translate to treatment plans:
Ovulation disorders—medication (clomiphene, letrozole) to stimulate egg release
Tubal blockages or damage—surgical repair or IVF bypass
Diminished ovarian reserve—specialized protocols, possibly combining approaches
Male factor infertility—sperm enhancement strategies or assisted reproduction
Uterine abnormalities—surgical correction before pursuing pregnancy
Unexplained infertility—empiric treatment or advanced procedures
Your specific diagnosis determines which path makes sense. Multiple factors sometimes require combined strategies.
Here’s how different results can direct specific treatment options:
Diagnosis | Usual First-Line Treatment | When Advanced Options Are Needed |
Ovulation Disorder | Ovulation-stimulating medication | If not responsive to meds |
Tubal Blockage | Surgical repair or IVF | If repair fails, move to IVF |
Male Factor Infertility | Sperm enhancement techniques | IVF with ICSI for severe cases |
Uterine Abnormality | Surgical correction | Repeat treatment if persists |
Unexplained Infertility | Lifestyle or IUI, then IVF | IVF after less invasive fails |
Why Personalization Matters
Treatment approaches vary based on evaluation findings, ranging from simple lifestyle changes to advanced fertility procedures. A woman over 35 with normal ovarian reserve needs a different strategy than one with significantly diminished reserve.
Age, medical history, and test results all influence recommendations. Your specialist weighs these factors alongside your preferences and timeline. Some patients prefer minimal intervention initially; others want aggressive treatment. Both approaches can work with proper planning.
Building Your Plan: Key Considerations
Your personalized plan addresses:
Your specific diagnosis—what tests revealed about your fertility
Your age and egg quality—urgency and treatment options available
Your medical history—prior conditions affecting approach
Your preferences—how aggressive or conservative you want to be
Success rates for your situation—realistic expectations based on your diagnosis
Costs and burdens—financial and emotional considerations
A good fertility specialist explains each element. You should understand why specific tests were ordered, what results mean, and how recommendations follow logically from findings.
Personalized fertility plans based on comprehensive workup results dramatically improve success rates compared to generic approaches.
Adjusting Plans Along the Way
Fertility treatment isn’t static. Monitoring during treatment allows specialists to adjust protocols based on how you respond. If standard medication doesn’t trigger ovulation, dosage increases or medication changes. If initial cycles don’t yield expected egg numbers, protocols shift.
This flexibility maximizes your chances while minimizing unnecessary treatment burdens.
Pro tip: Ask your specialist to explain the specific reasoning behind each recommendation—understanding the “why” helps you feel confident in your personalized plan and recognize when adjustments make sense.
Costs, Risks, and What to Expect Next
A fertility workup requires investment—financial, emotional, and time-wise. Understanding what you’ll spend, potential risks, and realistic timelines helps you prepare mentally and practically. Being informed prevents surprises and builds confidence in your journey.
Financial Considerations
Workup costs vary dramatically based on location, clinic, and insurance coverage. Basic bloodwork may cost $200-$500. Ultrasounds add $300-$800 per session. Imaging tests like HSG or hysteroscopy range from $1,000-$3,000 each.
Total workup expenses typically fall between $2,000-$5,000 without insurance. With insurance, you may pay copays or meet deductibles instead. Coverage varies wildly—some plans cover everything; others cover nothing.
Before scheduling, ask your clinic for itemized cost estimates. Contact your insurance company about coverage specifics. Many clinics offer payment plans if costs concern you.
Understanding the Risks
Most workup procedures carry minimal risks. Blood tests involve needle discomfort—occasionally bruising or infection, but extremely rare. Transvaginal ultrasound poses no significant risk; it’s simply uncomfortable for some.
Fertility evaluation procedures may involve discomfort or infection risks. HSG carries small infection risk and occasional allergic reaction to dye. Hysteroscopy requires anesthesia and carries standard surgical risks including infection and perforation—though serious complications occur in less than 1% of procedures.
Your specialist discusses specific risks before each procedure. Most people tolerate workup procedures well.
The Stepwise Approach: Why It Matters
Testing follows a stepwise progression from basic to advanced procedures as needed. You don’t jump to invasive testing immediately. Initial bloodwork and ultrasound reveal most common issues. Only if results warrant it do you progress to more advanced imaging.
This logical sequence:
Minimizes unnecessary procedures
Controls costs effectively
Reduces overall risk exposure
Often identifies problems quickly
Timeline Expectations
A complete workup typically takes 2-4 months from start to finish. Bloodwork happens early in your cycle. Ultrasound follows. If imaging is needed, HSG or sonohysterogram occurs mid-cycle. More complex testing takes additional weeks.
Your specialist may overlap some testing to move faster. If results point to needing a specialist referral, that adds time for scheduling and consultation.
After Your Workup: What Comes Next
Once testing completes, your clinic schedules a results consultation. This appointment is crucial—your specialist explains findings, answers questions, and discusses treatment options.
Three paths typically follow:
Simple treatment at your current clinic—medication or behavioral changes
Proceeding with treatment locally—IUI or other assisted procedures
Referral to fertility specialists—for complex cases needing advanced expertise
Understanding costs, risks, and timelines before starting your workup prevents anxiety and helps you plan accordingly.
Preparing for Your Consultation
Bring written questions to your results appointment. Ask about success rates for your specific diagnosis. Understand recommended treatment, alternatives, and expected costs. Request copies of all test results and imaging.
Don’t hesitate asking for clarification. A good specialist ensures you understand everything before proceeding.
Pro tip: Request your test results in writing before your consultation appointment, allowing time to review findings and prepare specific questions rather than hearing everything for the first time during the visit.
Take Control of Your Fertility Journey with Expert Guidance
Understanding the complexities of a fertility workup and dispelling common myths is the first step toward achieving your dream of parenthood. If you are facing challenges such as diminished ovarian reserve, ovulation disorders, or male factor infertility, personalized care is essential. At Rejuvenating Fertility Center, we specialize in comprehensive evaluations and innovative treatments tailored to your unique diagnosis. Our team, led by Dr. Zaher Merhi, employs advanced reproductive medicine including ovarian rejuvenation, IVF, and regenerative therapies to maximize your chances of success.
Don’t let unanswered questions or delayed diagnosis hold you back any longer. Visit Rejuvenating Fertility Center to explore our full range of fertility services and wellness programs designed for women over 35 and others seeking fertility preservation. Take the next step by booking a consultation so we can develop a personalized plan based on your fertility workup results. Your journey toward parenthood deserves cutting-edge care and unwavering support—start today at Rejuvenating Fertility Center.
Frequently Asked Questions
What is included in a fertility workup?
A fertility workup typically includes a review of medical and reproductive history, a physical examination, fertility testing (such as hormone levels and semen analysis), and evaluation of family history to identify potential causes of infertility.
How do I know if I need a fertility workup?
If you have been trying to conceive for 12 months without success (or 6 months if you are over 35), it is advisable to seek a fertility workup to explore underlying causes of infertility.
Why is timing important when considering a fertility workup?
Timing is crucial because age affects egg quality and quantity. For women over 35, starting the workup after 6 months of trying can help identify issues sooner, increasing the chances of successful treatment.
What common myths can delay fertility diagnosis?
Common myths include the belief that infertility is solely a woman’s issue, that age is the only cause of infertility, that IVF is the only solution, and that weight does not impact fertility. These misconceptions can prevent timely diagnosis and treatment.
Recommended